
A report in the New York Times on July 24th — Take Coronavirus More Seriously, Say Olympic Rowers Who Got It — casts important new light on the question, “when can we row.” In March, approximately one-third of the women’s national team contracted COVID-19 at the national training facility in NJ and months later some of the rowers were still feeling the effects.” With growing evidence that transmission is overwhelmingly airborne — not though surface contacts — and that healthy, young adults are at risk of serious complications from the disease, the experience of the US national rowing team should send a cautionary note to rowers and teams. There are significant unknown questions about COVID-19 transmission in general, but the belief that rowing is inherently safe because it is an outdoor sport needs re-examination. The people infected at the NJ training center were not just healthy, young adults; they were among the strongest and healthiest of young adults. Yet, as Olympic gold medalist Emily Regan said, “The narrative that has been going around in some places is that you won’t get the virus if you’re young and strong, or if you get it, it won’t be bad, but we’re perfect examples of how that is totally not true,”
On May 1st most federal restrictions relating to COVID-19 and social activities expired and approximately thirty states began relaxing their restrictions. In most states it is now (probably) legal to row. That doesn’t mean it’s safe; it only means it’s legal. [A comprehensive list of state restrictions can be found at the Council of State Governments website (https://web.csg.org/covid19/) and more information is available on our COVID-19 page.]
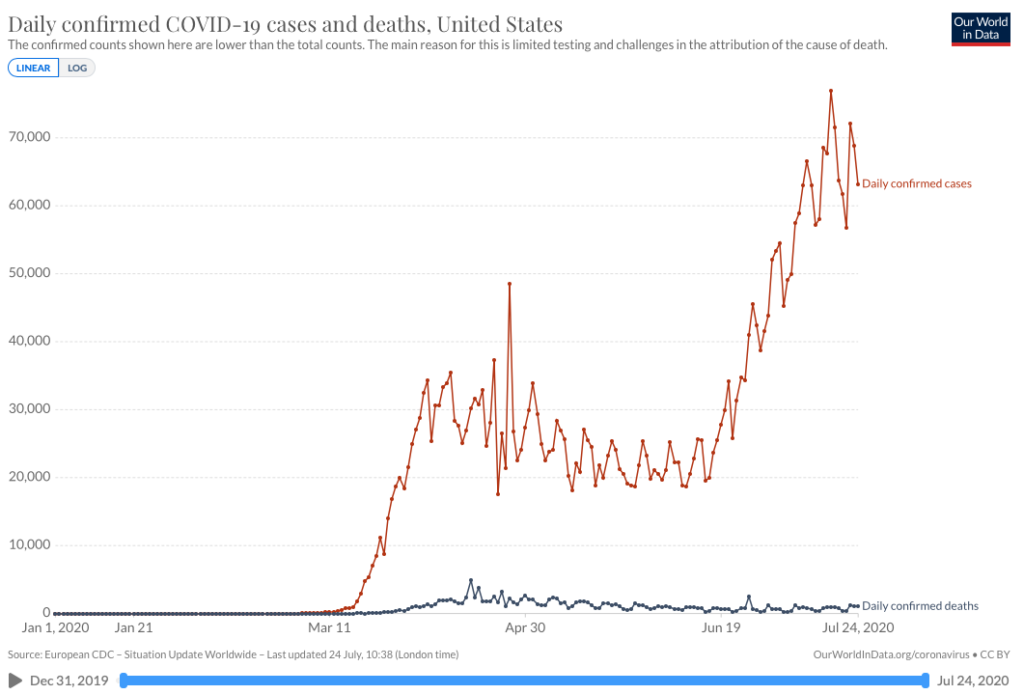
Following the relaxation of federal and state restrictions on activities throughout May, confirmed COVID-19 cases and deaths in the United States began resurging in the middle of June.
There are three sets of competing interests to consider when deciding whether or not to resume rowing with clubs and teams: political, economic, and medical. In theory, coordination between the three should optimize the social interest. In reality, political pressures to reopen the economy — however well justified — pose serious threats to the public health and to individuals.
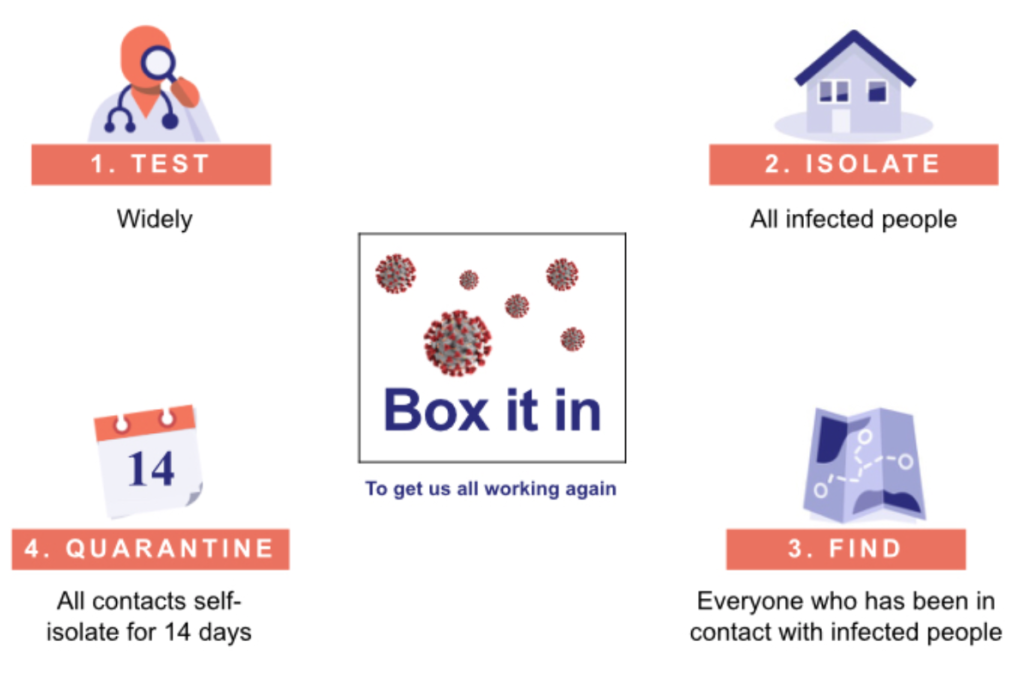
The consensus of the medical community — including virologists, epidemiologists, and medical historians — is heavily weighted against the resumption of social activities until the virus is constrained by these four criteria: 1) testing widely for COVID-19; 2) isolating all people who have tested positive or show symptoms of COVID-19; 3) identifying and finding everyone who has been in contact with infected people; and 4) quarantining both infected people and everyone who has been in contact with them for 14 days. These criteria are politically hard to meet; but they represent the consensus of medical thinking.
The number of confirmed COVID-19 cases in the United States as of May 6th is approximately 1,200,000; the number of deaths is over 71,000 and it is likely that the actual number of COVID-19 related deaths is substantially higher than the confirmed deaths (due to the fact that no tests were performed for COVID-19 in deaths attributed to other apparent causes).
———————————————————————————————————————-
On April 1st the head of the U.S. Centers for Disease Control and Prevention (CDC) warned that it is preparing “for another wave that we would anticipate in the late fall, early winter.[i]
On April 6th, articles were published in both Scientific American and The New York Times asking experts for their opinions about the timeline for resuming normal activities – including rowing. Two days later a third opinion was offered by the Chief Healthcare Officer of the Association of American Medical Colleges in Politico Magazine.[ii]
The Scientific American[iii] article was based on a report by the American Enterprise Institute and prepared by a team of medical doctors.[iv] It advocates a four-phase approach for resuming normal activities beginning with 1) better, systemic, testing and data analysis, and treatments; 2) A state by state response “when they are able to safely diagnose, treat, and isolate COVID-19 cases and their contacts;” 3) lifting social distancing restrictions “when safe and effective tools for mitigating the risk of COVID-19;” and 4) “investment into research and development initiatives, expansion of public-health and health care infrastructure and workforce, and clear governance structures to execute strong preparedness plans.”
In providing a measurement tool for the initial assessment, the Scientific American article suggested that “any given state that’s considering relaxing social distancing should have a demonstrated downward trend in cases over the two weeks prior… if the state has 500 new cases at its peak in a day, then the target should be that, for two weeks in a row, new cases drop daily—450, 400, 350, 300.”
The New York Times article was based on interviews with more than a dozen economists.[v] Essentially there was “a broad consensus on the building blocks the economy needs – but does not yet have – to begin the slow process of restoring normalcy in the American economy;” and they agreed that “there won’t be a fully functioning economy again until people are confident that they can go about their business without a high risk of catching the virus.”
With more than 15,000 Americans dead from the virus and ten million people thrown out of work, there is no agreement on when that might be. Moreover, there is no clear way to reconcile the goals of economists with the goals of the virus.
Drawing on the experience with the worldwide Influenza pandemic of 1918-1919, in which it is estimated that one-third of the world’s population became infected and 50 million people may have died, Dr. Janis Orlowski has cautioned that if we return “to a semi-normal life at the end of May… we have to prepare ourselves to go through a similar exercise in the fall… (when) we are (probably) going to go through this again.”
Ten Facts You Should Know Before Resuming Rowing
1. COVID-19 is a new disease. Human beings have no immunity for this disease. There are no effective treatments, no vaccines, and the United States continues to lag in the development and distribution of test kits necessary to contain the disease.
2. COVID-19 is highly contagious. The disease can be spread through direct contact between human beings or surface contact with contaminated objects. The primary vector, however, is through the aerosols dispersed in normal breathing, coughing, and sneezing, which may be spread up to twenty feet or more and remain airborne for hours. Most face masks do not prevent the virus from entering your nose and mouth but can reduce the risk. For this reason it is essential to wash frequently with soap and water.
3. COVID-19 symptoms vary widely and carriers may be asymptomatic. The most common symptoms resemble common diseases: fever: fatigue, cough, aches and pains, runny nose, sore throat, and shortness of breath. As many as half of all infected people may show no symptoms but still transmit the disease.
4. COVID-19 is deadly. Between March 1st and April 20th more than 40,000 Americans died from the disease. That is greater than the number of American combat soldiers who died in Vietnam from 1965 through 1968 (36,340) and the number who died on D-Day in World War II (6,603). More Americans are now dying daily from COVID-19 than died on 9/11.
5. The United States is now the epicenter of this global pandemic. It has had more cases of COVID-19 (>750,000) and more deaths (>40,000) than any other county and these numbers are continuing to rise. There is no indication it is subsiding or under control.
6. All COVID-19 data is preliminary and may underestimate the actual numbers. Because the disease is so new, all numbers regarding infections and deaths are subject to revision. Because so many people appear to be asymptomatic, or have mild symptoms, there are likely to be many more carriers of the disease than the confirmednumber of cases indicate. Similarly, deaths from pneumonia and other respiratory diseases may conceal more deaths linked to COVID-19.
7. Social Distancing doesn’t prevent COVID-19 transmission. It reduces the risk. Models of aerosol dispersion for runners, cyclists, and from coughing and sneezing indicate viral droplets may extend twenty to twenty-five feet from their source.
8. Exercise strengthens immunity. Because the white blood cells and proteins used to rebuild muscles after strenuous workouts are also used to fight diseases, exercise is generally healthy and bolsters immunity. Overexertion, however, without allowing recovery time, may weaken immunity.
9. There is likely to be a second wave of infections. Viruses persist and mutate. In the absence of an effective vaccine epidemiologists expect there is likely to be a second wave of infections (and deaths) in the fall. It is possible, as was the case with the flu epidemic of 1918-19, that the virus may become more lethal as a result of mutations.
10. There are no facts about the future. No one can predict the future of this disease but there seems to be a growing consensus among epidemiologists of four steps necessary to control it: 1) we must test widely for COVID-19; 2) everyone who tests positive or shows symptoms must be isolated; 3) everyone who has been in contact with infected people must be located; and 4) infected people and everyone who has been in contact with them must be quarantined for 14 days.
[i] Kashmira Gander, “CDC Director Says There May Be Anoth3r Coronavirus Wave I Late Fall…”, Newsweek, April 1, 2020. https://www.newsweek.com/cdc-director-coronavirus-wave-late-fall-substantial-portion-americans-will-susceptible-1495401
[ii] Zack Stanton, “‘By December, we are going to go through this again’,” Politico, 8 April 2020. https://www.politico.com/news/2020/04/08/coronavirus-when-normal-expert-health-care-172005
[iii] Tanya Lewis, “Pandemic Restrictions? Not Before Taking These Steps,” Scientific American, 6 April, 2020. https://www.scientificamerican.com/article/when-can-we-lift-the-coronavirus-pandemic-restrictions-not-before-taking-these-steps/
[iv] Scott Gottlieb, MD, et al., “National Coronavirus Response: A Road Map to Reopening,” American Enterprise Institute, 28 March, 2020. https://www.aei.org/wp-content/uploads/2020/03/National-Coronavirus-Response-a-Road-Map-to-Recovering-2.pdf
[v] Tim Tankersley, “U.S. Is Nowhere Close to Reopening the Economy, Experts Say,” New York Times, 6 April 2020. https://www.nytimes.com/2020/04/06/business/economy/coronavirus-economy.html?algo=top_conversion&fellback=false&imp_id=935726231&imp_id=58307207&action=click&module=Most%20Popular&pgtype=Homepage